Vitamin D Testing
![]()
Effective Date: October 30, 2019
Recommendations and Topics
- Scope
- Key Recommendations
- Definition
- Testing
- Recommended Vitamin D Intake
- Vitamin D Supplementation
- Monitoring
- Controversies in Care
- Resources
Scope
This guideline addresses the appropriate use of vitamin D testing in the general population in British Columbia, including children.
Recommendations on vitamin D dietary intake, supplementation and a brief section on the controversies surrounding vitamin D supplementation and clinical benefits are also included.
Key Recommendations
- Routine vitamin D testing or screening for vitamin D deficiency is not recommended.
- Measurement of vitamin D levels is not generally required prior to or after initiating vitamin D supplementation.
- Vitamin D testing is indicated in patients who are at high risk for vitamin D deficiency such as those with malabsorption syndromes, renal failure, unexplained bone pain, unusual fractures, or other evidence of metabolic bone disorders.
Definition
Vitamin D is a fat-soluble vitamin that stimulates intestinal calcium and phosphate absorption and is important in maintaining adequate blood calcium levels for bone mineralization, bone growth and remodelling. Vitamin D is also involved in the regulation of cell growth and metabolism, modulation of immune function, and reduction of inflammation. 1

Testing
Vitamin D testing is of low clinical utility for patients who are already suspected to be at risk of having suboptimal vitamin D levels and who would benefit from vitamin D supplementation.
Vitamin D testing is clinically indicated in patients with certain conditions predisposing them to vitamin D deficiency. These patients are generally managed by a specialist.
Vitamin D testing is only covered under the BC Medical Services Plan (MSP) when the patient is <19 years or when the test is ordered by a specialist.
Patients who relay requests from private healthcare practitioners to obtain vitamin D testing should be informed of the uncertain evidence supporting it. For a patient-friendly discussion on unnecessary testing and obtaining adequate vitamin D, refer to the resources listed under the Patient and Caregiver Resources section.
Vitamin D, in this context, refers to both vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) (See Appendix A: Synthesis and Metabolism of Vitamin D).2 Circulating forms of vitamin D2 and vitamin D3 include:
- 25(OH)D2 and 25(OH)D3 (referred to as 25-hydroxyvitamin D or 25(OH)D) which are the best biomarkers of nutritional vitamin D status and have a half-life of 2 weeks.
- 1,25(OH)2D2 and 1,25(OH)2D3 (referred to as 1,25-dihydroxyvitamin D) which are the biologically active forms of vitamin D and are not useful measures of vitamin D status because of their short half-life (15 hr).
25-hydroxyvitamin D (25(OH)D)
25(OH)D is the preferred test for assessing vitamin D status. Measuring 25(OH)D is the best way to determine the adequacy of vitamin D production by skin (D3) and oral intake (D2 or D3).
The test may be considered in the following clinical scenarios: 3
- significant liver disease
- significant renal disease
- osteomalacia
- osteopenia or osteoporosis
- history of non-traumatic (“fragility”) fractures
- malabsorption syndromes
- hypo- or hypercalcemia/hyperphosphatemia
- hypo- or hyperparathyroidism
- medications affecting vitamin D metabolism (e.g. phenobarbital, carbamazepine, phenytoin and valproate)
- unexplained elevation of alkaline phosphatase
- high dose vitamin D combined with evidence of vitamin D toxicity
There are a variety of testing methods measuring total serum 25(OH)D and to minimize assay variation, international reference standards have been developed.7 There is substantial assay variation which contributes to the lack of consensus on the laboratory values defining vitamin D deficiency. 7
|
25(OH)D Levels and Health 1, 4–6 |
|
|---|---|
|
<30 nmol/L |
Risk of vitamin D deficiency (rickets or osteomalacia) |
|
30-50 nmol/L |
Clinical features of inadequacy in some individuals |
|
≥50 nmol/L |
Adequate for bone health in practically all individuals |
|
> 125 nmol/L |
Potential for adverse effects |
1,25-dihydroxyvitamin D (1,25(OH)2D)
1,25(OH)2D should not be used for the investigation of vitamin D nutritional status. Measurement of 1,25 dihydroxyvitamin D levels is recommended only in isolated circumstances such as the investigation of parathyroid hormone independent hypercalcemia. 9
|
Vitamin D Tests in British Columbia |
||
|---|---|---|
|
MSP Cost of Tests8 |
||
|
Test Name |
Fee Item |
Cost |
|
25(OH)D |
92460 |
$61.32 |
|
1,25(OH)2D |
92455 |
$94.49 |
Current to January 1st, 2019
Vitamin D testing is only covered under the BC Medical Services Plan (MSP) when the patient is <19 years or when the test is ordered by a specialist.
Recommended Vitamin D Intake
Health Canada’s current recommended dietary allowances (RDAs) for vitamin D are based on maintenance of skeletal health. The RDAs listed in Table 1 below are adequate for 97.5% of Canadian residents. 1,6
Vitamin D and Your Health
-
On average, Canadian adults do not obtain sufficient vitamin D from dietary sources to meet the current RDA of 600 to 800 IU. Infants, children and older adults are especially prone to have inadequate dietary intake of vitamin D.6
The only significant natural food sources of vitamin D are fatty fish (e.g. salmon, mackerel, tuna) and egg yolks. There are no plant sources that provide a significant amount of vitamin D naturally. The major dietary sources of vitamin D are fortified foods. In Canada, cow’s milk and margarine are fortified with vitamin D. Goat’s milk, plant based beverages (e.g. soy and rice beverage), may also be fortified with vitamin D. Cheese and yogurt can be made with vitamin D-fortified milk, but do not contain as much vitamin D as milk alone.6
- For more information on dietary sources of vitamin D, see www.healthlinkbc.ca/healthlinkbc-files/vitamin-d-and- your-health (available in English, Chinese, Farsi, French, Korean, Punjabi, Spanish and Vietnamese). Primary care practitioners can recommend patients call 811 to speak to a HealthLink BC registered dietitian for additional information.
Exposure to Sunlight
The amount of vitamin D produced by the skin is dependent on the surface area exposed, skin pigmentation, age, season, latitude, cloud cover, time of day and use of sun screen. Adequate vitamin D can be made endogenously by careful exposure of the arms and legs to sunlight for 10-15 minutes per day in the summer months (See Appendix A: Synthesis and Metabolism of Vitamin D).10 However, deliberately increasing sun exposure to prevent vitamin D deficiency is not generally recommended due to the increased risk of skin cancer associated with UVA and UVB radiation. Glass blocks UVB and hence exposure to sunlight through glass does not lead to vitamin D synthesis. Use of tanning beds which emit primarily UVA is also not recommended to obtain adequate vitamin D.11
Vitamin D Supplementation
During the Canadian autumn, winter and spring, the adult population is unlikely to achieve adequate vitamin D levels through diet and sunlight alone. According to the 2011 Canadian Health Measures Survey, only about 68% of Canadians had levels > 50 nmol/L of vitamin D (levels adequate to prevent clinical insufficiency in majority of individuals). About one third of Canadians report taking a supplement containing vitamin D. Eighty five percent of Canadians who took a supplement were reported to have vitamin D levels > 50 nmol/L compared to 59% of non-supplement users.12
Since vitamin D supplementation in the general adult population is safe, it is reasonable to advise year-round supplementation without testing. It is important to advise patients against taking higher than recommended doses of vitamin D supplements – see Table 1 Daily Recommended Dietary Allowance for Vitamin D and Vitamin D Toxicity. Vitamin D supplements are almost always contraindicated for individuals with hypercalcemia and should be used with caution in people with hyperphosphatemia.
- Newborns: Human breast milk contains low levels of vitamin D and infants who drink less than 1000 mL of vitamin D fortified infant formula may not receive enough vitamin D. A daily vitamin D supplement of 400 IU (10 µg) from birth to 24 months of age is recommended. Refer to the Vitamin D Recommendations for Perinatal Women & Healthy Term Infants (Birth - 1 year) Practice Support Tool for Health Professionals in British Columbia available at www2.gov.bc.ca/assets/gov/ health/managing-your-health/healthy-eating/vitamin-d-practice-support-tool.pdf
- Pregnancy and Lactation: Vitamin D supplementation of 400 IU (10 µg) to 600 IU (15 µg) daily during pregnancy and lactation is recommended. Refer to the Vitamin D Recommendations for Perinatal Women & Healthy Term Infants(Birth - 1 year) Practice Support Tool for Health Professionals in British Columbia available at www2.gov.bc.ca/assets/gov/ health/managing-your-health/healthy-eating/vitamin-d-practice-support-tool.pdf
- Midlife and Older Adults often do not consume enough vitamin D rich food, and in addition, aging reduces the efficiency with which the skin synthesizes vitamin D and the kidney’s ability to convert vitamin D to its active form. Health Canada recommends that adults greater than 50 years take a supplement of 400 IU daily to help achieve their RDA. Adults> 70 years have a higher RDA of 800 IU.1, 6 For those in long term care facilities a daily supplement of 800 IU to 2000 IU is recommended.13
Dosage and Form
The two major forms of vitamin D supplements are available as D2 (ergocalciferol) or D3 (cholecalciferol). Most over-the-counter supplements available in Canada contain vitamin D3. Vitamin D3 doses over 1000 IU/dosage or where the recommended daily dose would result in more than 1000 IU/day (such as liquid forms) require a prescription. Although vitamin D2 is available in Canada over-the-counter and by prescription, use of vitamin D3 over vitamin D2 is recommended as vitamin D3 has been shown to be three times more effective than vitamin D2 at increasing serum 25(OH)D levels and maintaining these levels over a longer period of time. 14, 15
Vitamin D3 supplements are available over the counter in a variety of strengths and dosage forms, including tablets, capsules, sprays and drops (drops are recommended for infants and children under age 4). Tablets and capsules are available as 400 and 1000 IU vitamin D3. Many multivitamins sold in Canada also contain vitamin D3, typically ranging from 400-1000 IU/day.
Weekly dosing forms or monthly dosing forms are available and may be more convenient for some patients and have been shown to be safe.16 Administration of high dose vitamin D3 once a year is not recommended, as evidence has shown possible increased fracture risk.17
Vitamin D and Calcium for Bone Health in Postmenopausal Women and Older Men
Post-menopausal women and older men have traditionally been recommended 800 IU/day of vitamin D due to their increased risk of osteoporosis and osteoporotic fractures. This recommendation has been questioned. A recent meta-analysis reported no effect on the risk of fractures or falls and bone mineral density with vitamin D supplementation in community-dwelling women age 65 years or older.18 The US Preventative Task Force (2018) concluded that the current evidence is inconclusive to assess the benefits and harms of supplementation with vitamin D alone or in combination with calcium for the primary prevention of fractures in community-dwelling postmenopausal women and asymptomatic men.19 However, considering the strengths and limitations of the analyses, Osteoporosis Canada maintains that individuals with osteoporosis or with risk factors for fractures receive adequate vitamin D, recommended at 800-2,000 IU/day. 20, 21
- For specific recommendations for patients at risk of osteoporosis, see the associated guideline at BCGuidelines.ca: Osteoporosis – Diagnosis, Treatment and Fracture Prevention.
Vitamin D Toxicity
Since vitamin D is fat soluble, excessive intake can lead to accumulation and cause toxicity by way of hypercalcemia (typically at levels > 250 nmol/L) and its associated sequelae. Plasma concentrations of > 375 nmol/L of 25(OH)D pose significant risk of vitamin D toxicity.22, 23 The Institute of Medicine advises vitamin D intakes greater than 4000 IU/day may cause renal impairment, hypercalcemia or vascular calcification.1
Vitamin D toxicity and resultant hypercalcemia (typically at levels > 250 nmol/L) can have neuropsychiatric effects (e.g., confusion, depression, psychosis, stupor), gastrointestinal effects (e.g., recurrent vomiting, abdominal pain, anorexia, constipation, peptic ulcers, pancreatitis), cardiovascular manifestations (e.g., hypertension, arrhythmia), and renal effects (e.g., hypercalciuria, polyuria, polydipsia, dehydration, nephrocalcinosis, and renal failure).22
- If there is a clinical suspicion of excessive vitamin D intake, the recommended testing for hypervitaminosis D is serum calcium (total or ionized) with a concomitantly collected parathyroid (PTH) hormone. If calcium is high and PTH is low, vitamin D testing should be arranged either by referral to a specialist or through consultation with a laboratory physician.
Monitoring
Testing vitamin D levels is not indicated prior to or after starting routine vitamin D supplementation.
Routine monitoring of vitamin D following supplementation is only indicated to assess dosage adequacy in patients with clinical conditions managed by a specialist (e.g. renal disease, metabolic bone disease, malabsorption syndromes).
Controversies in Care
In recent years, rates of vitamin D testing and sales of vitamin D supplements have increased significantly. However, despite the ongoing clinical and research interests in vitamin D, there continues to be controversy and, in some cases, contradictory evidence. While long established as essential for bone health, vitamin D has also been increasingly promoted for the prevention of a range of other conditions including cancer, cardiovascular disease, diabetes, autoimmune disorders, and cognitive decline. However, much of this evidence is based on observational data; association between vitamin D levels and clinical outcomes is inconsistent among studies and subject to confounding biases. 24–26 Large scale studies are exploring these associations and may help establish the role of vitamin D and non-skeletal effects.
Resources
References
- Office of Dietary Supplements - Vitamin D [Internet]. [cited 2019 Mar 28]. Available from: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- Sempos CT, Heijboer AC, Bikle DD, Bollerslev J, Bouillon R, Brannon PM, et al. Vitamin D assays and the definition of hypovitaminosis D: results from the First International Conference on Controversies in Vitamin D: Vitamin D assays and defining hypovitaminosis D. Br J Clin Pharmacol. 2018 Oct;84(10):2194–207.
- Canadian Agency for Drugs and Technologies in Health (CADTH). Vitamin D Testing in the General Population: A Review of the Clinical and Cost Effectiveness and Guidelines (2015). [Internet]. Available from: https://www.cadth.ca/sites/default/files/pdf/htis/jan-2015/RC0626%20Vitamin%20D%20Testing%20Final.pdf
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D [Internet]. Ross AC, Taylor CL, Yaktine AL, Del Valle HB, editors. Washington (DC): National Academies Press (US); 2011 [cited 2019 Oct 4]. (The National Academies Collection: Reports funded by National Institutes of Health). Available from: http://www.ncbi.nlm.nih.gov/books/NBK56070/
- LeFevre ML, LeFevre NM. Vitamin D Screening and Supplementation in Community-Dwelling Adults: Common Questions and Answers. Am Fam Physician. 2018 Feb 15;97(4):254–60.
- Health Canada. Vitamin D and Calcium: Updated Dietary Reference Intakes (2019). [Internet]. Available from: https://www.canada.ca/en/health-canada/services/ food-nutrition/healthy-eating/vitamins-minerals/vitamin-calcium-updated-dietary-reference-intakes-nutrition.html
- Lucas RM, Gorman S, Black L, Neale RE. Clinical, Research, and Public Health Implications of Poor Measurement of Vitamin D Status. J AOAC Int. 2017 Sep 1;100(5):1225–9.
- Laboratory Services Outpatient Payment Schedule [Internet]. Available from: http://www.bccss.org/clinical-services/bcaplm/health-professionals/outpatient- payment-schedule
- BCGuidelines. Hormone Testing – Indications and Appropriate Use (2016). [Internet]. Available from: https://www2.gov.bc.ca/gov/content/health/practitioner- professional-resources/bc-guidelines/special-endocrine-testing
- Hossein-nezhad A, Holick MF. Vitamin D for Health: A Global Perspective. Mayo Clin Proc. 2013 Jul;88(7):720–55.
- Vanchinathan V, Lim HW. A Dermatologist’s Perspective on Vitamin D. Mayo Clin Proc. 2012 Apr;87(4):372–80.
- Janz T, Pearson C. Vitamin D blood levels of Canadians [Internet]. Statistics Canada; [cited 2017 Dec 13]. Report No.: 82-624–X. Available from: https://www.statcan. gc.ca/pub/82-624-x/2013001/article/11727-eng.htm
- Papaioannou A, Santesso N, Morin SN, Feldman S, Adachi JD, Crilly R, et al. Recommendations for preventing fracture in long-term care. CMAJ Can Med Assoc J. 2015 Oct 20;187(15):1135–44.
- Tripkovic L, Lambert H, Hart K, Smith CP, Bucca G, Penson S, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. 2012 Jun;95(6):1357–64.
- Toyn C, Darling AL, Hart K, Tripkovic L, Smith CP, Mathers JC, et al. Effect of vitamin d2 supplementation on serum 25 hydroxy-vitamin d3 levels: a systematic review and meta-analysis. Proc Nutr Soc [Internet]. 2018 ed [cited 2019 Apr 8];77(OCE1). Available from: https://www.cambridge.org/core/journals/proceedings-of-the-nutrition- society/article/effect-of-vitamin-d2-supplementation-on-serum-25-hydroxyvitamin-d3-levels-a-systematic-review-and-metaanalysis/C3489970DF534383A3C1EC5318 016B0D
- Canadian Agency for Drugs and Technologies in Health (CADTH). Calcium and Vitamin D Supplementation for Adults: Safety and Guidelines (2018). [Internet]. Available from: https://www.cadth.ca/sites/default/files/pdf/htis/2018/RB1229%20Calcium%20and%20Vitamin%20D%20Final.pdf
- Sanders KM, Stuart AL, Williamson EJ, Simpson JA, Kotowicz MA, Young D, et al. Annual High-Dose Oral Vitamin D and Falls and Fractures in Older Women: A Randomized Controlled Trial. JAMA. 2010 May 12;303(18):1815.
- Bolland MJ, Grey A, Avenell A. Effects of vitamin D supplementation on musculoskeletal health: a systematic review, meta-analysis, and trial sequential analysis. Lancet Diabetes Endocrinol. 2018 Nov;6(11):847–58.
- US Preventive Services Task Force, Grossman DC, Curry SJ, Owens DK, Barry MJ, Caughey AB, et al. Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2018 Apr 17;319(15):1592.
- Osteoporosis Canada. Vitamin D and effects on fractures, falls and bone mineral density (2018). [Internet]. Available from: https://osteoporosis.ca/vitamin-d-and- effects-on-fractures-falls-and-bone-mineral-density/
- Hanley DA, Cranney A, Jones G, Whiting SJ, Leslie WD, Cole DEC, et al. Vitamin D in adult health and disease: a review and guideline statement from Osteoporosis Canada. Can Med Assoc J. 2010 Sep 7;182(12):E610–8.
- Marcinowska-Suchowierska E, Kupisz-Urbańska M, Łukaszkiewicz J, Płudowski P, Jones G. Vitamin D Toxicity–A Clinical Perspective. Front Endocrinol [Internet]. 2018 Sep 20 [cited 2019 Mar 29];9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6158375/
- Galior K, Grebe S, Singh R. Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients [Internet]. 2018 Jul 24 [cited 2019 Mar 29];10(8). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6115827/
- Manson JE, Bassuk SS. Vitamin D Research and Clinical Practice: At a Crossroads. JAMA. 2015 Apr 7;313(13):1311.
- Pilz S, Zittermann A, Trummer C, Theiler-Schwetz V, Lerchbaum E, Keppel MH, et al. Vitamin D testing and treatment: a narrative review of current evidence. Endocr Connect. 2019 Feb;R27–43.
- Manson JE, Cook NR, Lee I-M, Christen W, Bassuk SS, Mora S, et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N Engl J Med. 2019 Jan 3;380(1):33–44.
Abbreviations
25(OH)D: 25-hydroxyvitamin D
1,25(OH)2D: 1,25-dihydroxyvitamin D
RDAs: recommended dietary allowances
Practitioner Resources
- RACE: Rapid Access to Consultative Expertise Program – www.raceconnect.ca
A telephone consultation line for select specialty services for physicians, nurse practitioners and medical residents.
If the relevant specialty area is available through your local RACE line, please contact them first. Contact your local RACE line for the list of available specialty areas. If your local RACE line does not cover the relevant specialty service or there is no local RACE line in your area, or to access Provincial Services, please contact the Vancouver Coastal Health Region/Providence Health Care RACE line.- Vancouver Coastal Health Region/Providence Health Care: www.raceconnect.ca
Available Monday to Friday, 8 am to 5 pm
604 696-2131 (Vancouver area) or 1 877 696-2131 (toll free) - Northern RACE: 1 877 605-7223 (toll free)
- Kootenay Boundary RACE: www.divisionsbc.ca/kb/race 1 844 365-7223 (toll free)
- Fraser Valley RACE: www.raceapp.ca (download at Apple and Android stores)
- South Island RACE: www.raceapp.ca (download at Apple and Android stores) or www.divisionsbc.ca/south-island/RACE
- Note that endocrinology on Vancouver Island is available through the Royal Jubilee Hospital/Victoria General Hospital on call endocrinologist. The on call endocrinologist can be reached through intranet.viha.ca or the Royal Jubilee Hospital switchboard.
- Vancouver Coastal Health Region/Providence Health Care: www.raceconnect.ca
- Pathways: PathwaysBC.ca
An online resource that allows GPs and nurse practitioners and their office staff to quickly access current and accurate referral information, including wait times and areas of expertise, for specialists and specialty clinics. In addition, Pathways makes available hundreds of patient and health-care practitioner resources that are categorized and searchable.
Patient and Caregiver Resources
- HealthLink BC (www.healthlinkbc.ca). You may call HealthLinkBC at 8-1-1 toll-free in B.C., or for the deaf and the hard of hearing, call 7-1-1. You will be connected with an English speaking health-service navigator, who can provide health and health-service information and connect you with a registered dietitian. Registered dietitians are available Monday to Friday, 9am to 5pm Pacific Time. Translation services are available in over 130 languages on request.
- Vitamin D Test – available at www.healthlinkbc.ca/medical-tests/abp2312#show-all
- Food sources of Calcium and Vitamin D – available at www.healthlinkbc.ca/healthlinkbc-files/vitamin-d
- Choosing Wisely: Vitamin D tests – available at choosingwiselycanada.org/vitamin-d-tests/
This guideline is based on scientific evidence current as of the effective date.
The guideline was developed by the Guidelines and Protocols Advisory Committee, in collaboration with BC’s Agency for Pathology and Laboratory Medicine and adopted by the Medical Services Commission.
For more information about how BC Guidelines are developed, refer to the GPAC Handbook available at BCGuidelines.ca: GPAC Handbook.
THE GUIDELINES AND PROTOCOLS ADVISORY COMMITTEE
|
The principles of the Guidelines and Protocols Advisory Committee are to:
Contact Information: Guidelines and Protocols Advisory Committee Disclaimer The Clinical Practice Guidelines (the guidelines) have been developed by the guidelines and Protocols Advisory Committee on behalf of the Medical Services Commission. The guidelines are intended to give an understanding of a clinical problem, and outline one or more preferred approaches to the investigation and management of the problem. The guidelines are not intended as a substitute for the advice or professional judgment of a health care professional, nor are they intended to be the only approach to the management of clinical problem. We cannot respond to patients or patient advocates requesting advice on issues related to medical conditions. If you need medical advice, please contact a health care professional. |
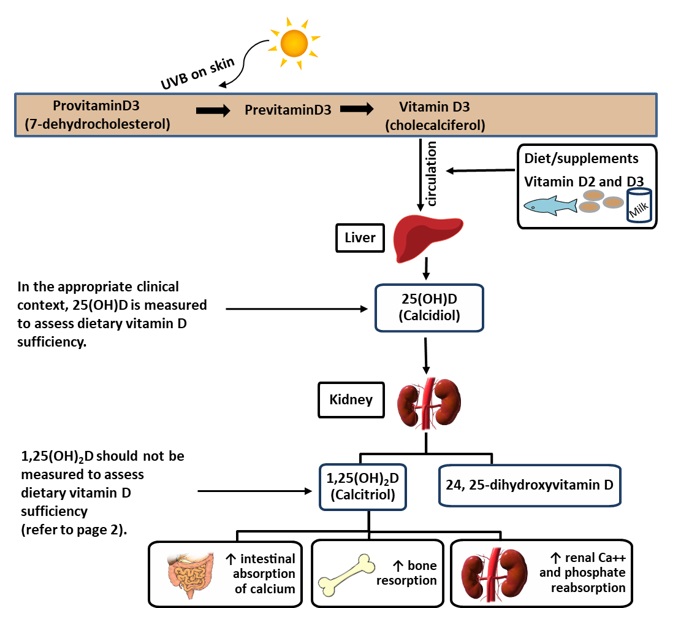
Appendix A – Synthesis and Metabolism of Vitamin D
Upon exposure to UVB radiation, previtamin D3 is synthesized from 7-dehydrocholesterol in the skin. Previtamin D3 isomerizes by body heat to form vitamin D3 (cholecalciferol). Vitamin D3 and vitamin D2 (obtained from diet and supplements) are then transported by the blood to the liver, where it is converted to 25-hydroxyvitamin D (25(OH)D). The active form of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)2D) is formed in the kidneys and is tightly regulated by the parathyroid hormone. The circulating plasma concentration of vitamin D, expressed as the sum of 25(OH)D2 and 25(OH)D3, is considered the best biomarker of nutritional vitamin D status. Although 1,25(OH)2D is the biologically active form, serum 1,25(OH)2D is not a useful measure of vitamin D status as it is frequently normal in the setting of vitamin D deficiency and because it has a short half-life (15 hr) compared to 25(OH)D which has a half-life of 2 weeks.2